Infantile Idiopathic Scoliosis
A 5-year case study of an Infantile Scoliosis Patient Using Schroth Therapy and Cheneau Type Scoliosis Brace
Introduction
The purpose of this case study is to present a description and timeline of applying Schroth therapy and Chêneau-type bracing using Rigo principles (a Rigo-Chêneau brace) for the conservative treatment of a boy with scoliosis from ages 3 to 8 years.
Conservative Treatment of Scoliosis
Scoliosis Bracing
Patients with infantile idiopathic scoliosis (IIS) and juvenile idiopathic scoliosis (JIS) who have large curve magnitudes, irrespective of the treatment method, have a high risk of curve progression.1 Therefore, the design, function, and fitting process of a scoliosis brace has to be well-thought-out. To accomplish this, complete a specific physical evaluation of the patient as outlined by the author in 2014.2 The result of this evaluation will guide the selection of the optimal brace type for the individual case. When the Rigo-Chêneau brace is chosen for young patients, it is essential to assemble an experienced team of scoliosis professionals that includes an orthopedic surgeon, a physical therapist trained in the Schroth Method, and an orthotist.
Case Presentation and Methods
A 6-month-old boy, who was born in October 2006, was diagnosed with scoliosis that presented with a left thoracic curve of 32 degrees Cobb angle. At the age of 22 months, he underwent surgery to correct a tethered spinal cord, which is believed to have contributed to the curve progression to 80 degrees Cobb angle. No treatment for scoliosis was applied from the time of diagnosis until after the surgery for the tethered spinal cord. Subsequent to the surgery, the spinal cord was detethered, allowing the spine to grow straighter and more naturally. As a result, the left thoracic curve reduced to 56 degrees Cobb angle. However, after a few months, the curve had regressed to 80 degrees Cobb angle.
In September 2009, physiotherapist Christa Lehnert-Schroth, PT, began coaching the then 3-year-old patient’s mother, prescribing case-specific exercises that the mother helped the boy to perform. In February 2011, the orthotist (and author of this article) fitted the patient with the first of five Rigo-Chêneau braces. The pre-brace Cobb angle for the main thoracic curve at that time was 71 degrees. The orthotist’s goal was to overcorrect in-brace posture and provide brace support while the patient strengthened atrophied muscle groups at home with his daily Schroth exercise regimen.
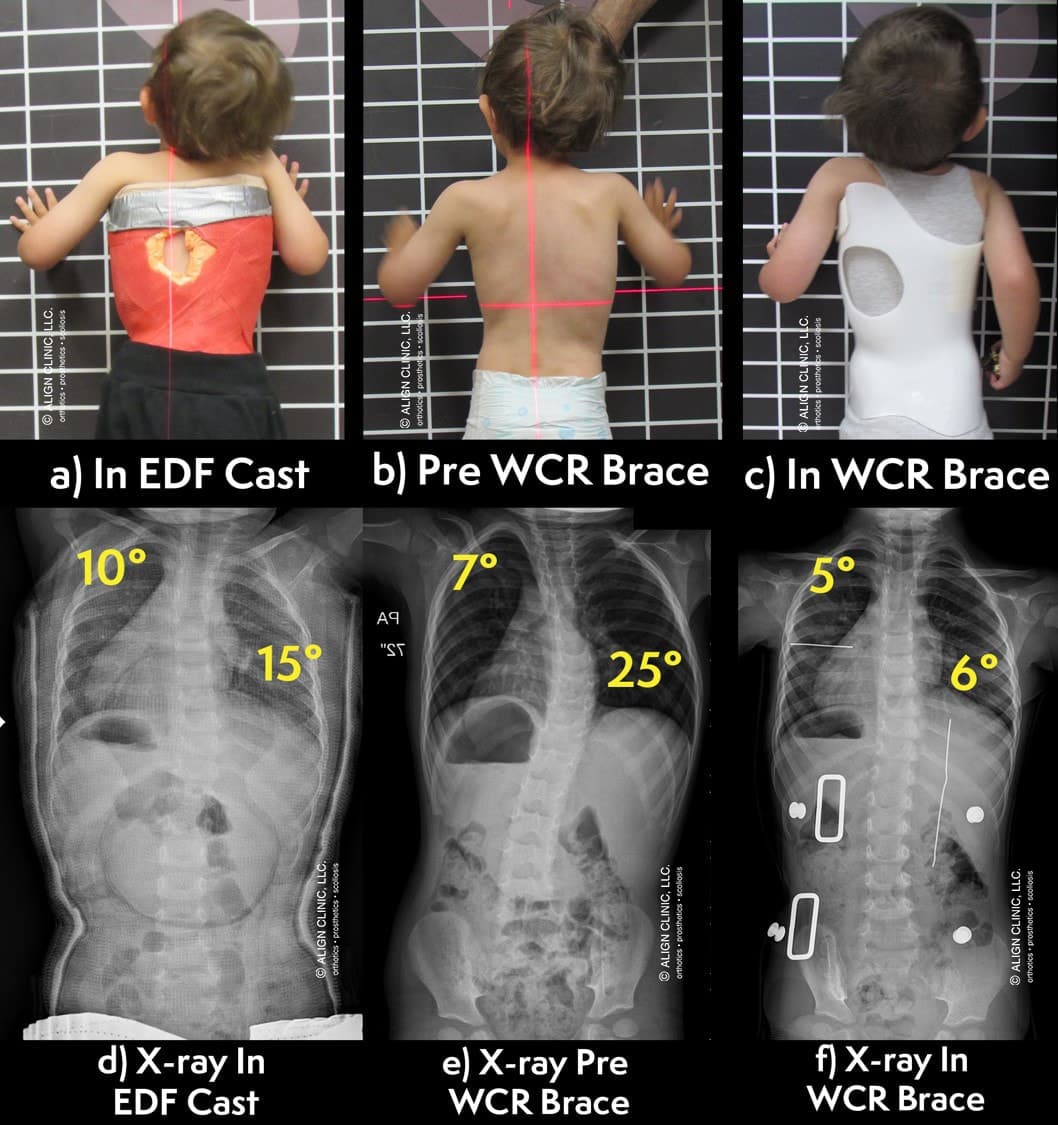
In 2011, at 4 years old, the patient presented with a three-curve scoliosis, A2 type with a D modifier, according to the Rigo classification of scoliosis.6 The trunk imbalance was to the convex major thoracic side with the collapse of the vertebral column on the concave side of the thoracic curve, and the shoulder was lower on the left side (Figure 1a). The dorsal left rib hump can be seen clearly in the clinical presentation. The Cobb angle of the main thoracolumbar curvature was 71 degrees with a proximal thoracic curve of 42 degrees prior to the start of the Rigo-Chêneau brace treatment (Figure 1b). In reference to the central sacral line (CSL), which is a vertical line from the center of the sacrum, the overhang was to the left and the prominence of the pelvis presented on the right (i.e. the trunk was translated to the left side and the pelvis was translated to the right side).
Literature Review
There are multiple reported cases of success with Schroth therapy and scoliosis bracing involving patients as young as 3 to 5 years old. During the Society on Scoliosis Orthopaedic and Rehabilitation Treatment (SOSORT) 2013 annual conference in Chicago, Lebel reported on a 5-year-old girl who was diagnosed with JIS. The patient had a thoracic curve of 53 degrees Cobb angle and a lumbar curve of 24 degrees Cobb angle. She started Schroth physiotherapy and scoliosis bracing at the age of 6 years. At 9 years old, the patient presented with a thoracic curve of 16 degrees Cobb angle out of brace. At the age of 10 years, she continued to show improvement of the scoliosis with reduction of the thoracic rotation as well as improved chest expansion. Lebel declared that, at that time, the patient had avoided undergoing eight to nine growing rod surgeries.4
At the SOSORT 2014 annual conference in Wiesbaden, Germany, Tomasz Kotwicki presented a case very similar to the case presented herein. Kotwicki reported on a 3.8-year-old boy who presented pre-brace with a left thoracic curve of 70 degrees Cobb angle that was reduced through conservative treatment to 40 degrees Cobb angle out of brace. This patient wore a Chêneau-type scoliosis brace for more than five years and engaged in physiotherapy that was Schroth-like but with more asymmetrical respiration and active self-correction. The patient presented with improvements in balance, rotation, and Cobb angle measurements at 8.6 years of age.5





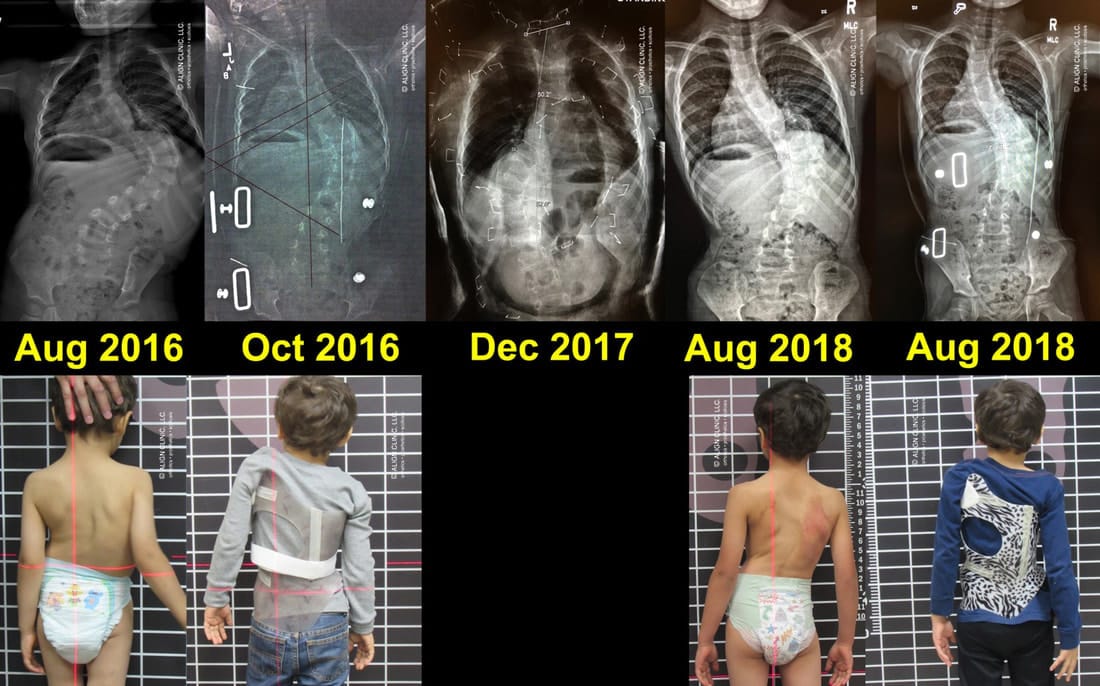
2B. Patient in first Rigo-Cheneau type brace in 2011
2C. Patient in 2011 after first brace
2D. Patient in 2013 after second brace
2E. Patient in third brace in 2014







Results
The Schroth therapy and the Rigo-Chêneau scoliosis brace reduced the patient’s Cobb angle by 48 percent out of brace from the 2011 pre-brace 71 degrees Cobb angle to the most recent x-ray (in 2015) of 37 degrees Cobb angle. A significant improvement in clinical presentation was also documented and observed.
Discussion
The patient had a good initial response to his first Rigo-Chêneau brace, with 46 percent in-brace correction. In 2012, the patient was able to hold some of the in-brace correction, which reduced the main thoracic curve from 71 degrees to 52 degrees out of brace. In 2013, the patient achieved a few more degrees of out-of-brace correction, to 48 degrees out of brace. The brace that was fabricated in 2013 was able to correct the main thoracic curve to 20 degrees, which represented a 72 percent in-brace correction. In 2014, the patient was able to hold some of the significant in-brace correction, and presented with a 32 degrees left thoracic curve. As a result, the left thoracic curve was smaller than the proximal thoracic curve.
From 2014 to 2015, the left thoracic Cobb angle increased from 32 degrees to 37 degrees, and the proximal upper structural curve decreased from 41 degrees Cobb angle to 39 degrees Cobb angle. This 5 degree increase of the left thoracic curve, in the author’s opinion, was due to the change in brace design. The decision to change the brace design of the thoracic region, specifically the area of the left thoracic pressure area, was to improve the contact of the brace to the ribs. It was noticed in the 2014 out-of-brace x-ray that the ribs on the convex thoracic side, specifically the 11th and 12th ribs, were more vertical. The negative effect of the verticalization of the ribs can be caused primarily by too much lateral pressure. Also, excessive lateral translation of the trunk to the right, over the pelvis, causes more frontal plane imbalance.
The patient had experienced significant improvements and changes in the clinical and x-ray presentations from the age of 4 years until 7 years. The x-ray in 2014 presented with a 55 percent out-of-brace correction, and the brace that the patient had worn for that past year produced a 72 percent in-brace correction of the main left thoracic Cobb angle. As a result, the design of the brace in 2014 focused less on achieving a big Cobb angle correction and rather on changing the orientation of the forces from the brace to the ribs, to better align the ribs horizontally on the convex thoracic side and to improve 3D correction of the patient. The change in pressures was important for the patient’s future ability to control the scoliosis during puberty. That is, pushing too much might cause the ribs to lose integrity and thus lose effectiveness in transmission of forces from the brace to the spine.
Conclusion
Although this patient would not normally be considered for scoliosis bracing, he clearly benefited from the Schroth therapy and Rigo-Chêneau brace treatment. This combination of conservative treatments significantly improved the clinical presentation (sagittal normalization, reduced rotation, and pelvis and trunk alignments) as well as the out-of-brace Cobb angle measurements. The patient’s mother was able to systematically apply and supervise Schroth exercises at home for more than five years, concurrent with utilization of the five Rigo-Chêneau braces, ultimately allowing the patient to live a completely normal and healthy life.
Future work is required to present the results of this patient after he goes through the periods of puberty and adolescence, during which the risk of curve progression is highest.
Grant Wood, MSc, CO, is the cofounder of Align Clinic, San Mateo, California, and vice chair of the Spinal Orthotics Society of the American Academy of Orthotists and Prosthetists. He is a specialist in scoliosis bracing with the Chêneau brace and the Wood-Chêneau-Rigo (WCR) brace.
Academy Society Spotlight is a presentation of clinical content by the Societies of the American Academy of Orthotists and Prosthetists in partnership with The O&P EDGE.
Acknowledgement
The author is grateful to the late Christa Lehnert-Schroth, PT, for her generous and compassionate efforts to facilitate a warm, therapeutic relationship between him, this patient, and the patient’s mother, which was invaluable for success of conservative treatment. He would also like to thank Manuel Rigo, MD, for the physical evaluation of this patient and contribution to the brace design.
In Memoriam: Christa Lehnert-Schroth, December 8, 1924-March 22, 2015
Christa Lehnert-Schroth, PT, devoted her entire life to treating patients with scoliosis. The daughter of Katharina Schroth, who had developed a system of physical therapy to halt and reverse scoliosis and related spinal deformities. She was an active participant in the management of the patient presented in this case study until the time of her death. Christa Lehnert-Schroth will be sorely missed and her spirit forever revered by many thousands of patients and therapists all over the world.GE.
References
- Wood, G. I. 2013. To brace or not to brace: The three-dimensional nature and growth considerations for adolescent idiopathic scoliosis. The Academy Today 9 (3):A-5-8.
- Wood, G. I. 2014. Bracing efficacy in the patient with idiopathic scoliosis: improvements in technique and care coordination. The Academy Today 10 (3):A-5-8.
- Lehnert-Schroth, Christa. 2007. Three-dimensional treatment for scoliosis: A physiotherapeutic method for deformities of the spine. Palo Alto, CA: The Martindale Press.
- Lebel, A. 2013. Preliminary result of 4 years of conservative management juvenile idiopathic scoliosis, A case report. Scoliosis 8 (Suppl. 2).
- Kotwicki, T. 2014. Case presentation at the annual meeting of the Society on Scoliosis Orthopaedic and Rehabilitation Treatment, Wiesbaden, Germany.
- Wood G. I. 2014. Reversing Scoliosis and brace treatment of a proximal structural curve. The O&P Edge 13 (3):60-4.